Figures
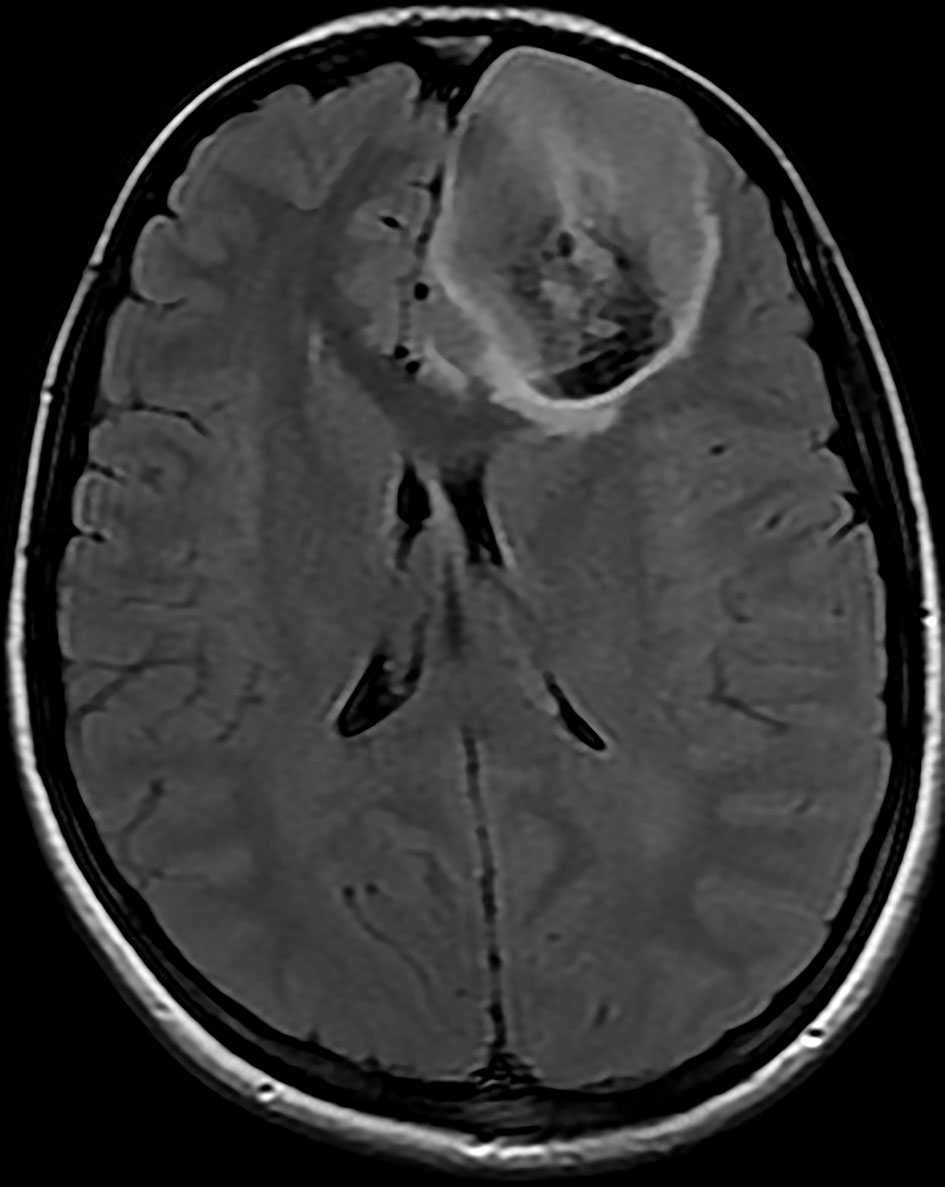
Figure 1. Brain MRI shows three left frontal cortical based lesions which appear hyperintense on T2 weighted image with mild mass effect but without significant vasogenic edema. The largest lesion shows inhomogeneity with cystic changes and modest enhancement after IV gadolinium administration with tiny ring enhancing focus which shows restricted diffusion. MRI: magnetic resonance imaging; IV: intravenous.
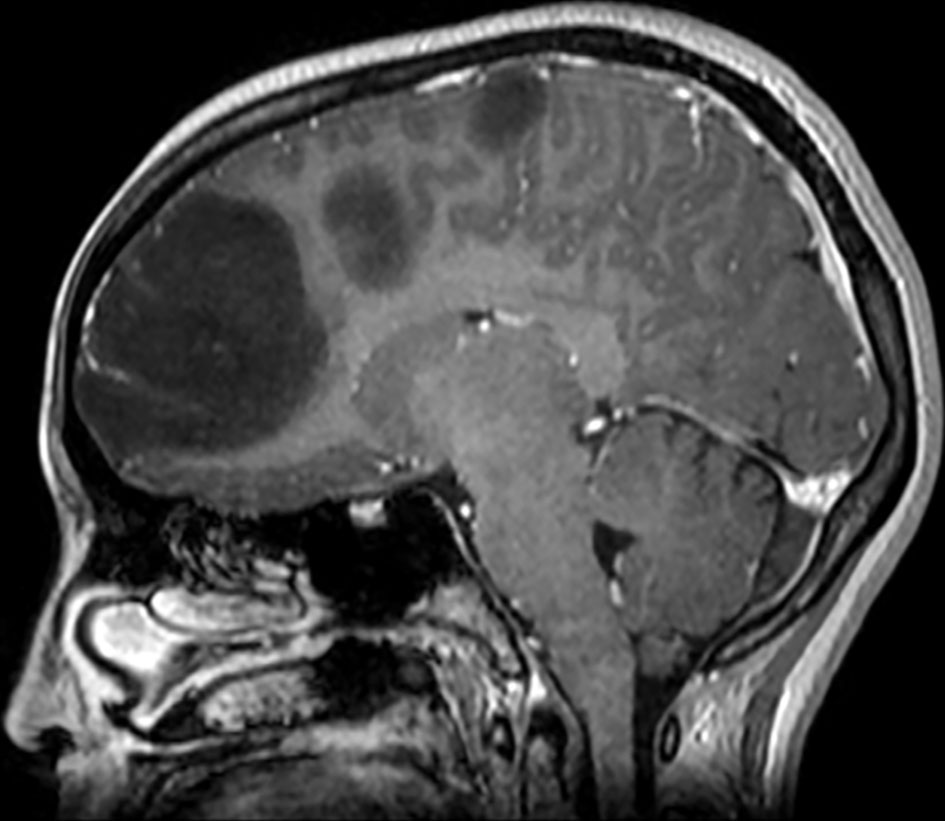
Figure 2. Brain MRI shows three left frontal cortical based lesions which appear hypointense on T1 weighted image. MRI: magnetic resonance imaging.
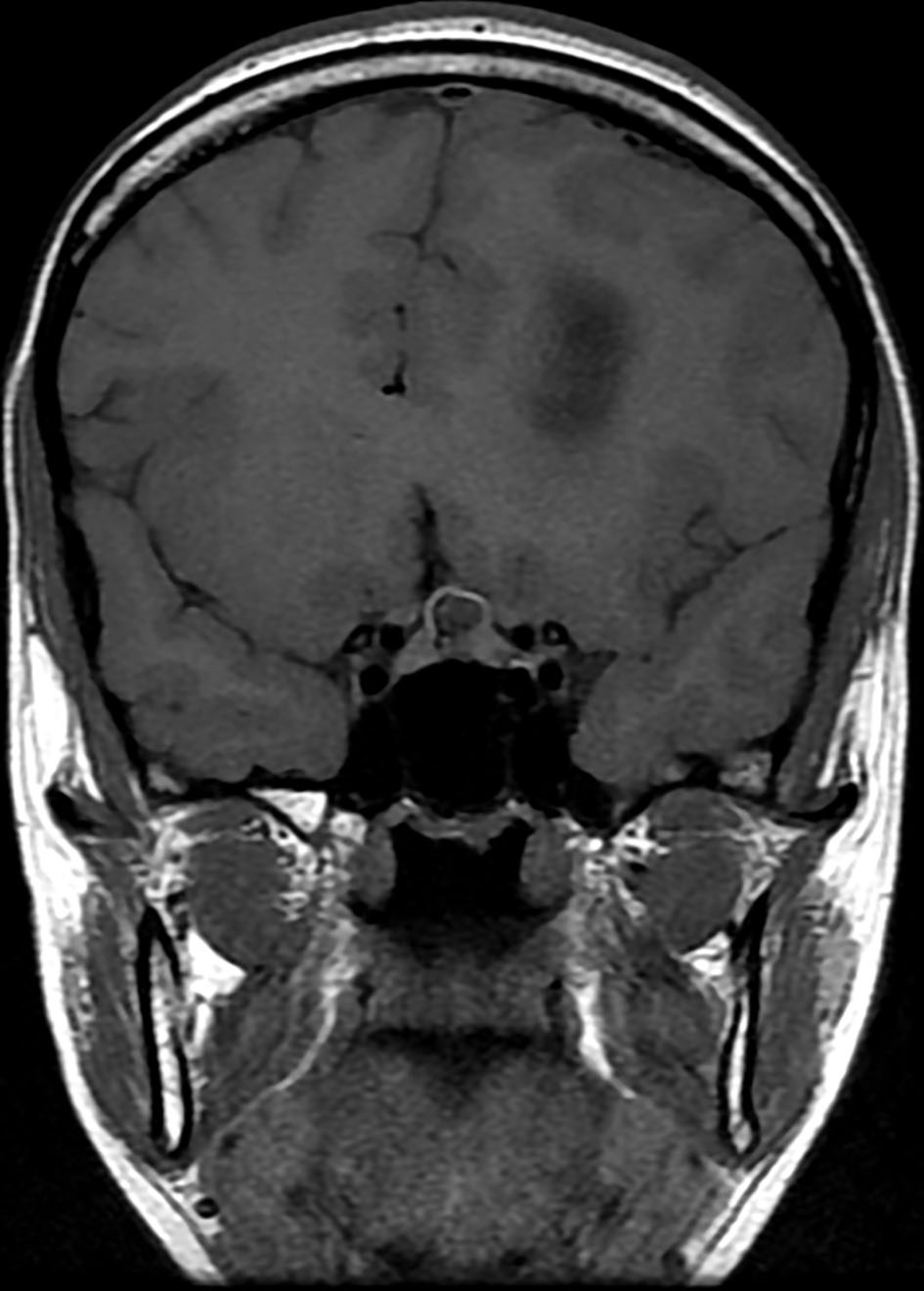
Figure 3. Brain MRI shows a small complex sellar lesion with anterior enhancing component. It is extending into the suprasellar cistern. MRI: magnetic resonance imaging.
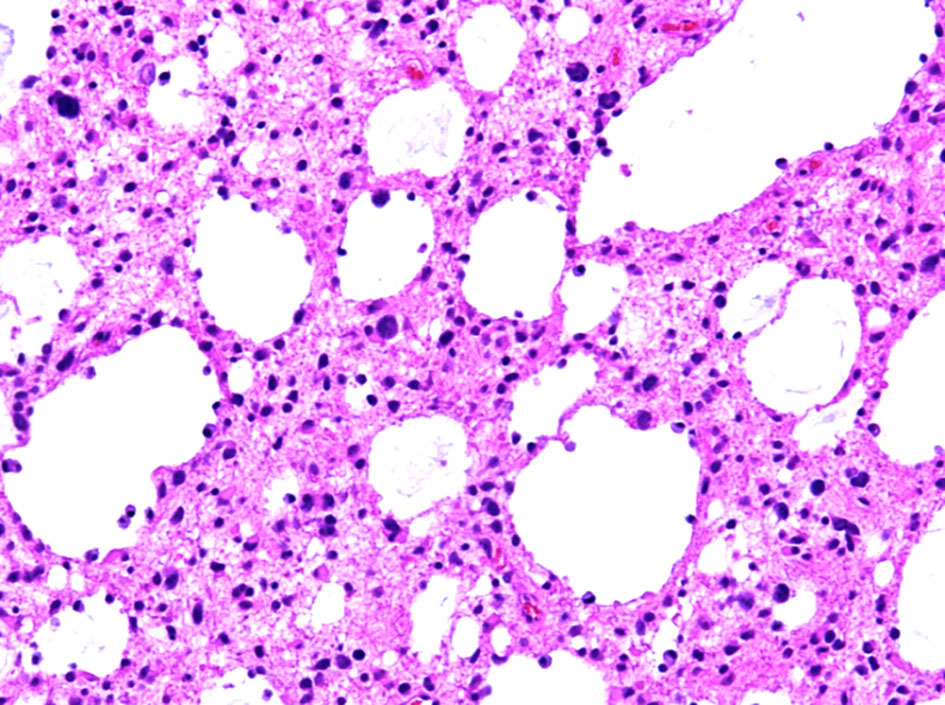
Figure 4. Histopathological examination of the diffuse astrocytoma specimen at intermediate power (× 20) shows an infiltrative growth pattern and microcytic changes.
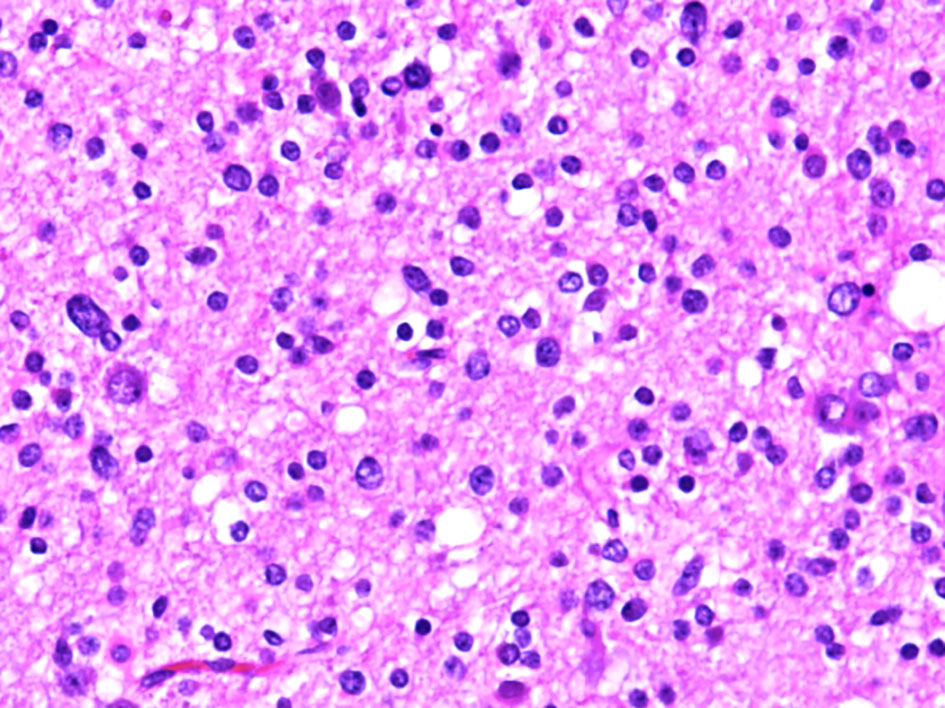
Figure 5. Histopathological examination of the diffuse astrocytoma specimen at high power (× 40) show a tumor cells have a more round and uniform appearance with microcytic changes.
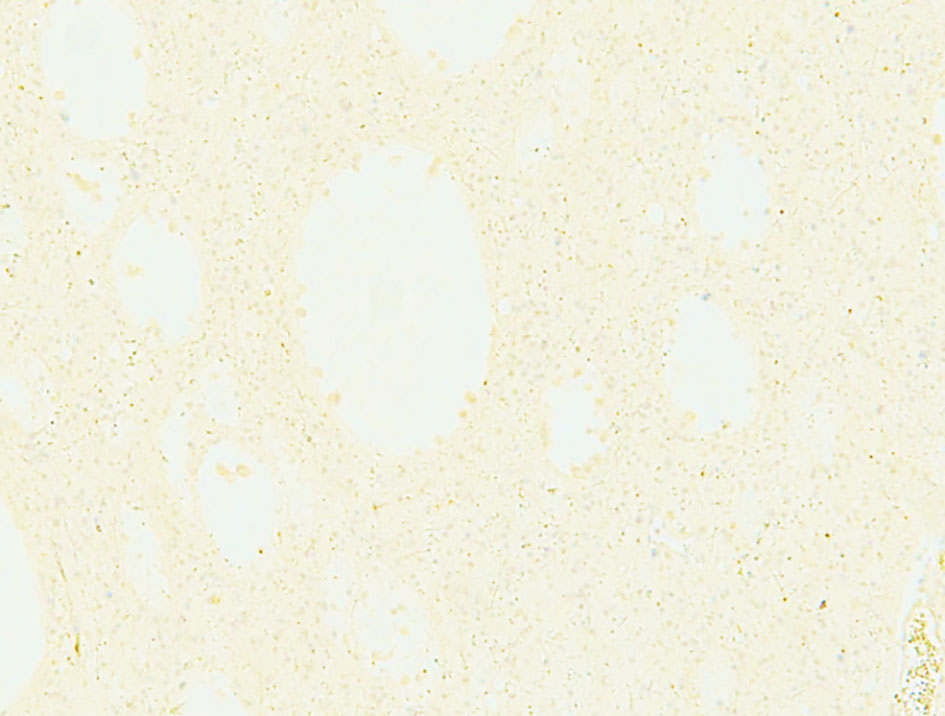
Figure 6. Negative immunohistochemical staining for IDH1. IDH1: isocitrate dehydrogenase 1.
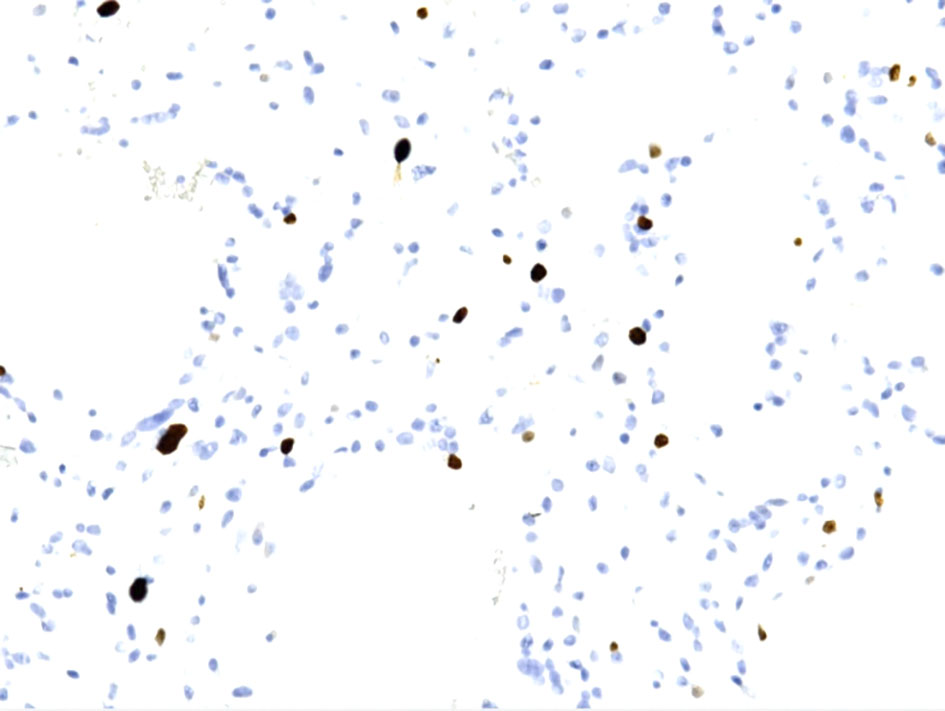
Figure 7. Ki67 immunohistochemical staining shows from low to focally moderate (up to 6-8%).

Figure 8. X-ray of the pelvis (AP view) shows ill-defined mixed lytic and sclerotic lesions with chondroid matrix, irregularity and bony destruction affecting mainly the left iliac bone and to a lesser extent the left inferior pubic ramus and the iliac side of the right SI joint. No periosteal reaction nor pathological fracture. AP: anteroposterior; SI: sacroiliac.
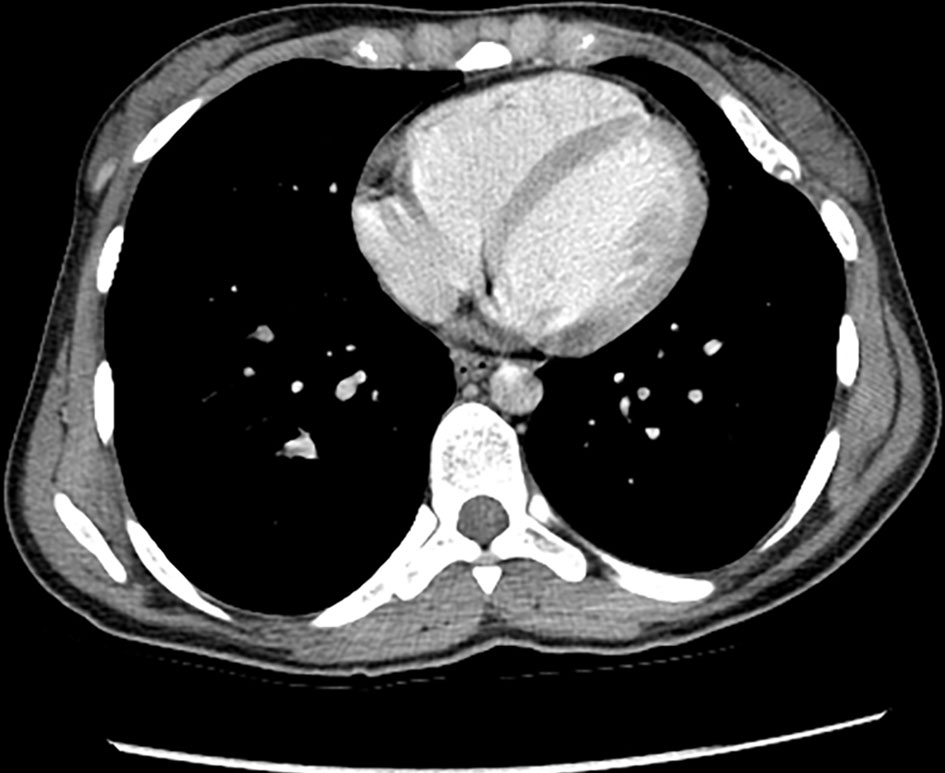
Figure 9. Enhanced chest CT (axial view) shows few nonspecific subpleural nodules in the left upper lobe. There are multiple osseous expansile lesions with popcorn type calcification. CT: computed tomography.
Table
Table 1. Twenty-Five Reported Cases in the Literature Including Our Patient Since 1979
| Studies | Case year | Age/gender | Histology |
|---|
| Bathla et al, 2012 [4] | 1979 | 26/NS | Grade II oligoastrocytoma |
| Bathla et al, 2012 [4] | 1987 | 38/M | Astrocytoma |
| Bathla et al, 2012 [4] | 1987 | 29/M | Anaplastic astrocytoma |
| Bathla et al, 2012 [4] | 1988 | 34/M | Grade II astrocytoma |
| Bathla et al, 2012 [4] | 1990 | 24/M | Low grade astrocytoma |
| Bathla et al, 2012 [4] | 1991 | 29/F | High grade astrocytoma |
| Bathla et al, 2012 [4] | 1994 | 23/M | Anaplastic astrocytoma |
| Bathla et al, 2012 [4] | 1994 | 25/M | Oligodendroglioma |
| Bathla et al, 2012 [4] | 1994 | 46/M | Oligoastrocytoma |
| Bathla et al, 2012 [4] | 1998 | 28/M | Low grade astrocytoma |
| Bathla et al, 2012 [4] | 1999 | 16/M | Diffuse brainstem (astrocytoma?) |
| Bathla et al, 2012 [4] | 1999 | 23/F | pons involvement (astrocytoma?) |
| Bathla et al, 2012 [4] | 1999 | 28/? | Low grade astrocytoma? |
| Bathla et al, 2012 [4] | 2002 | 7/F | Low grade astrocytoma |
| Bathla et al, 2012 [4] | 2004 | 21/F | Low grade fibrillary astrocytoma |
| Bathla et al, 2012 [4] | 2006 | 28/F | Anaplastic mixed oligoastrocytoma |
| Bathla et al, 2012 [4] | 2008 | 14/M | Anaplastic astrocytoma. |
| Bathla et al, 2012 [4] | 2009 | 6/F | Glioblastoma multiforme |
| Hori et al, 2010 [8] | 2010 | 4/M | Anaplastic astrocytoma |
| Bathla et al, 2012 [4] | 2010 | 19/M | Grade III anaplastic astrocytoma |
| Bathla et al, 2012 [4] | 2012 | 16/M | Grade II glioma |
| Khan et al, 2013 [7] | 2013 | 35/M | Low grade astrocytoma |
| Rebecca et al, 2016 [6] | 2016 | 26/M | Anaplastic oligodendroglioma |
| Gajavelli et al, 2016 [9] | 2016 | 55/F | Anaplastic astrocytoma |
| Present study | 2020 | 23/F | Grade II astrocytoma |