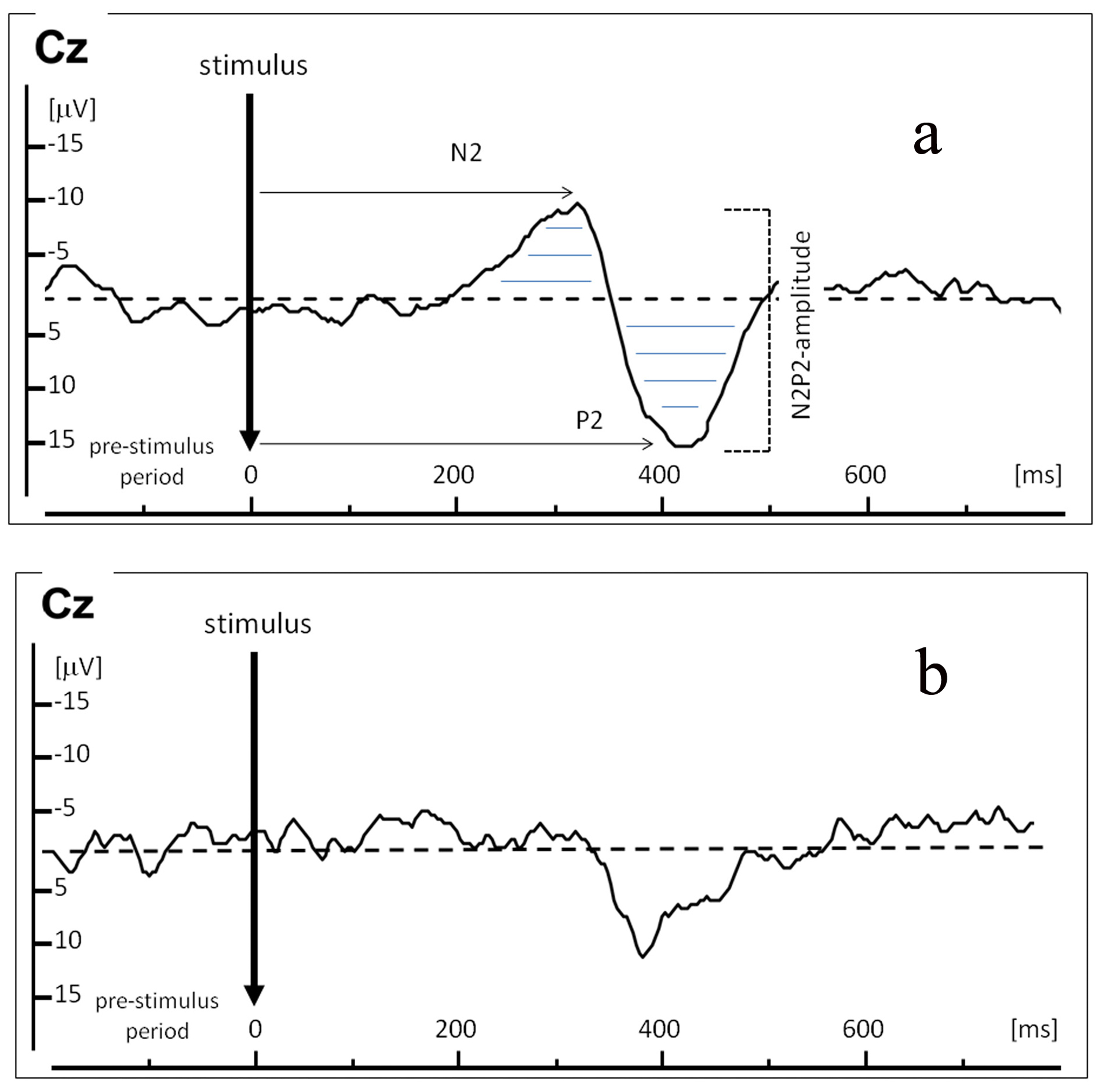
Figure 1. Example of a Laser Evoked Potential (LEP) recordings in one representative healthy control (a), and below an example of an attenuated LEP in one representative sarcoidosis patient in clinical remission with complaints of burning pain (b). X-axis represents time in ms; Y-axis represents amplitude in µV. LEP was recorded at electrode Cz. Arrows indicate N2-latency and P2-latency in ms; horizontal lines indicate N2P2-amplitude (µV) over time (ms).