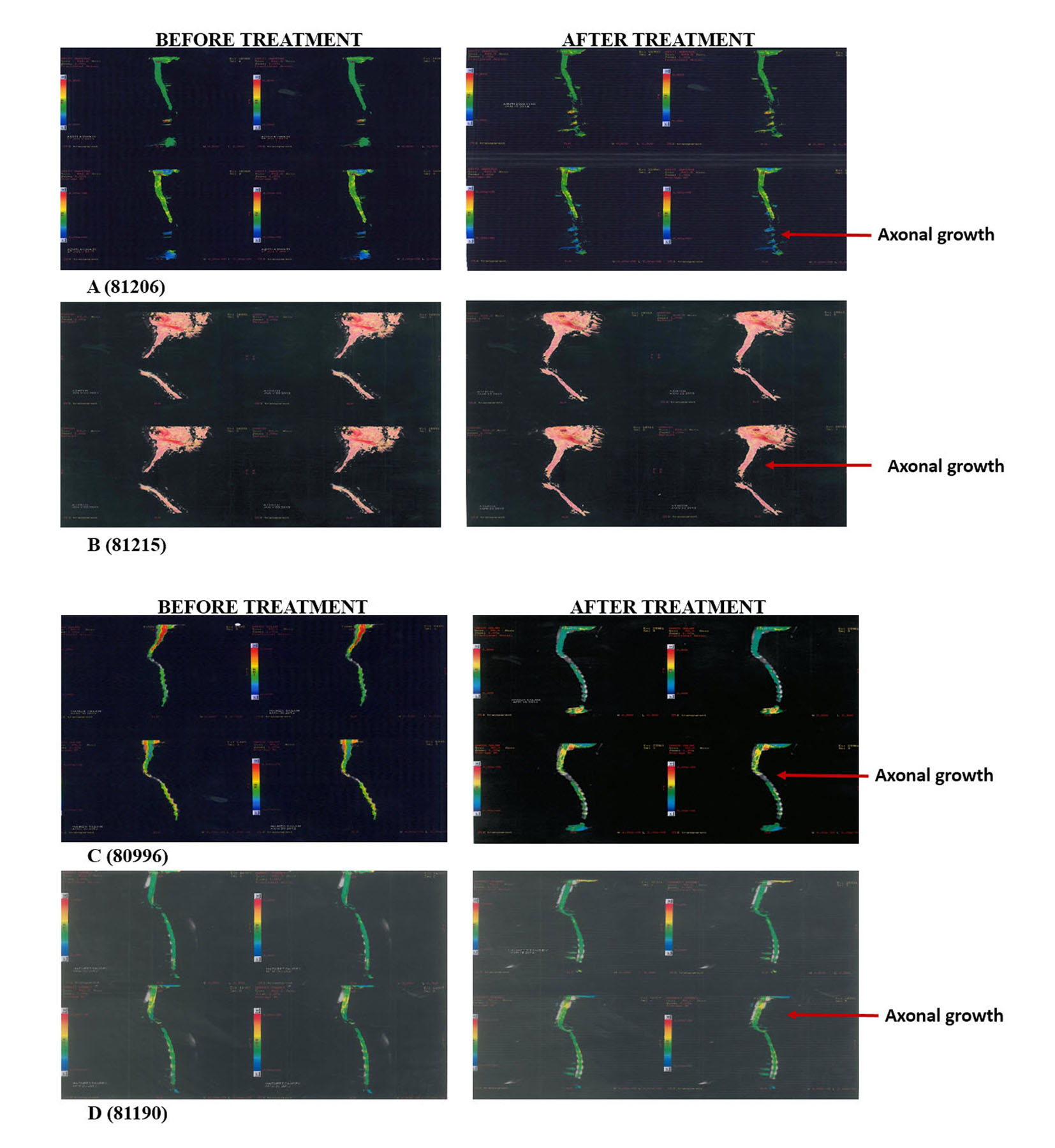
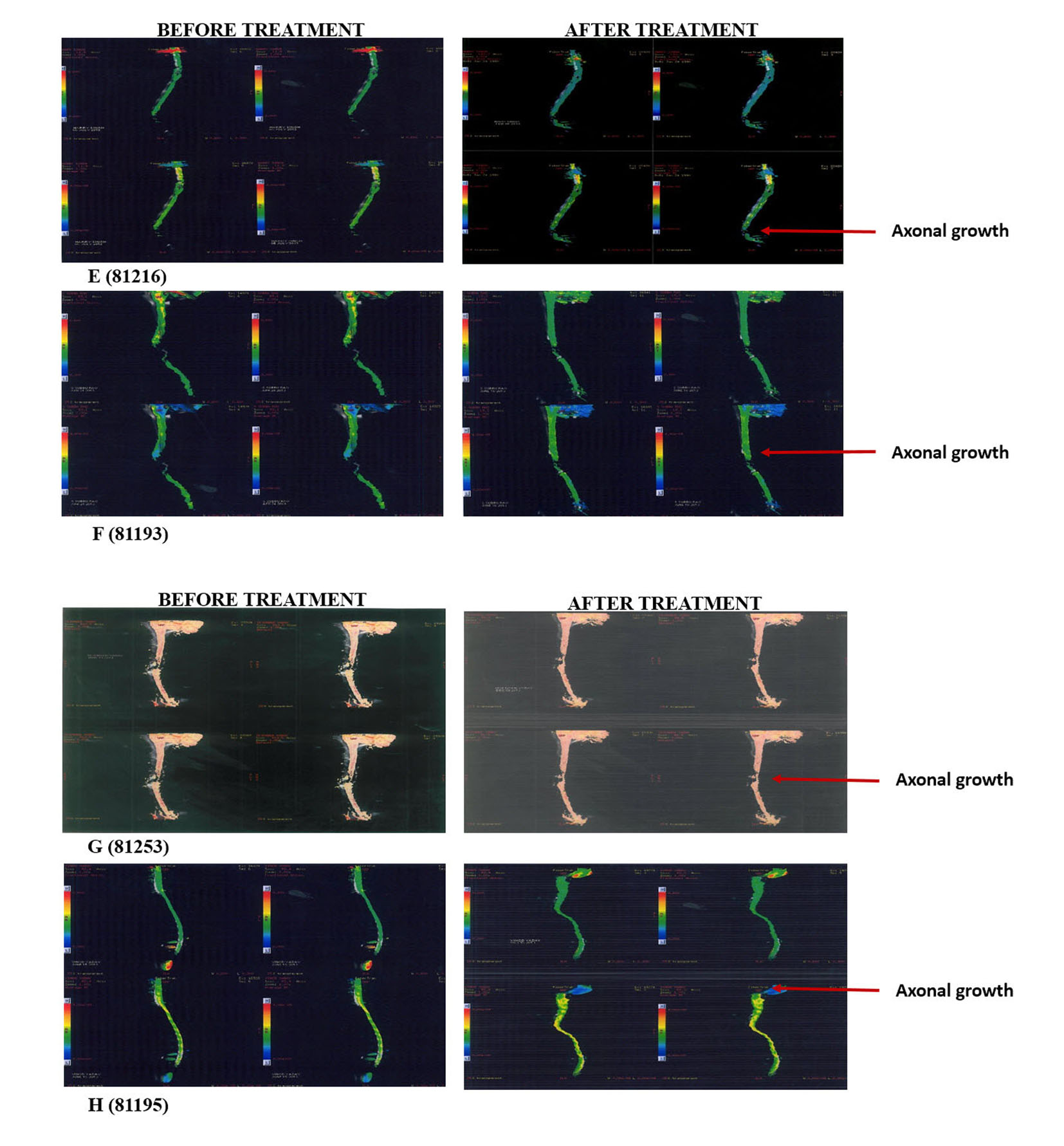
Figure 1. Tractography images of patients before and after hESC therapy.
| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website http://www.neurores.org |
Original Article
Volume 5, Number 3, June 2015, pages 213-220
Human Embryonic Stem Cells in Treatment of Spinal Cord Injury: A Prospective Study
Figure
Tables
| Patient No. | ASIA score | Treatment days | GAP phase days | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | |||||||
| Start | End | Start | End | Start | End | Start | End | |||
| 80996 | A | A | B | C | D | D | D | D | 215 | 207 |
| 81191 | C | C | C | C | D | D | 127 | 206 | ||
| 81192 | A | A | 54 | 0 | ||||||
| 81193 | C | C | C | C | 98 | 93 | ||||
| 81194 | B | B | C | C | 77 | 85 | ||||
| 81196 | A | A | 17 | 0 | ||||||
| 81206 | A | A | A | A | A | A | 421 | 170 | ||
| 81215 | A | A | 42 | 0 | ||||||
| 81216 | A | A | A | A | A | A | 111 | 320 | ||
| 81223 | A | A | A | A | A | A | 190 | 298 | ||
| 81253 | B | B | C | C | C | C | 121 | 167 | ||
| Patient No. | Radiological examinations (MRI and tractography) | |
|---|---|---|
| Before | After | |
| 81191 | There were interruption of cord nerve fibers at C6-C7 and C7-D1 level; no continuity of fibers was seen at level of myelomalacia changes. | There was irregularity of the cord outline at the level of myelomalacia change. The fibers continuity at the level of cord injury was better visualized. |
| 81193 | There was artifactual distortion with non-visualization of about two vertebral lengths of the spinal cord at the site of injury/metallic plate and screw fixation. | The artifactual distortion seen at C6 and C7 level with interrupted visualization of nerve fibers/tracts. No continuous bridging of the cranial and caudal ends of the normal cord was seen. |
| 81194 | The study revealed mild centromedullary hyperintensity in spinal cord at D6/D7 disc to D10 vertebral level. Fractional anisotropy maps show patchy reduction of FA values at D11-D12, D9-D10, D8-D9 and C7-D1 level. | The study revealed mild centromedullary hyperintensity in the spinal cord at D6/D7 disc to D10 vertebral level. Compared to the fractional anisotropy maps/values there was interval increase in the FA values at all levels from D7 to D12 level. |
| 81206 | There was marked thinning of the spinal cord at D7 to D12 level. The conus medullaris is moderately thinned and mild centromedullary hyperintensity was seen in the conus. There was non-visualization of the fiber tracts in the cord distal to D7 level. | There was non-visualization of the fiber tracts in the cord distal to D7 level. Marked thinning of the spinal cord was observed at D7 to D12 level on sagittal MRI sections. The conus medullaris was moderately thinned and mild centromedullary hyperintensity was seen in the conus. |
| 81215 | There was complete non-visualization of the cord tracts with abrupt cut off at the cranial end. | There was partial visualization of the cord tracts in the myelomalacia segment, progressively decreasing caudally with focal complete non-visualization at C6-C7 disc level. |
| 81216 | Ascending and descending white matter tracts were seen cephalic and caudal to the myelomalacia segment. At the level of myelomalacia cord changes, there was patchy visualization of tracts across the length of this segment. | Myelomalacia changes were seen in the spinal cord at lower D10 level with focal thinning. Caudal to this, up to D11-D12 disc level cystic myelomalacia changes were seen with expansion of cord contour and linear/irregular gliotic scars on the right side. |
| 81223 | The dorsal cord showed focal complete interruption of nerve fibers/tracts at D9 level with slight in-homogeneity. | The dorsal cord showed focal complete interruption of nerve fibers/tracts at the level of cord injury. There was no signification interval change in the MRI tractography. |
| 81253 | There was visualization of tracts/white matter fibers posterior in the myelomalacia segment in less than third of the cord AP width. Some focal areas of interruption were seen in cranial part of this posterior visualized parenchyma. | There was focal loss of visualization of tracts/white matter fibers in lower part of the myelomalacia segment. No continuous fiber visualization was seen in the myelomalacia segment. |
| Patient No. | Clinical status | |
|---|---|---|
| Before | After | |
| KAFO: knee-ankle-foot orthosis; AFO: ankle-foot orthosis; LE: lower extremity; B/L: bilateral. | ||
| 80996 | Loss of sensation below level of injury, no bowel/bladder sensation, B/L LE spasticity, unable to stand. | Sitting balance improved with good hip flexion range, improved sensation of right thigh, walking improved, spasticity reduced, and walks with B/L KAFO and walker, core strength improved. |
| 81191 | Unable to walk, weakness in right forearm, loss of sensation below nipples, no bowel/bladder control, unable to sit independently, right hand grip weak, can stand with knee gaiters for 3 - 4 min. | B/L LE power improved, intermittent flickers and sensation in B/L feet, calves; gait pattern and balance improved, sitting and standing balance improved, can crawl, knee sitting with some support, deep sensation and light touch improved till thigh. |
| 81192 | Cannot move lower limb, cannot sit or stand without support, stiffness in lower limbs, and no bowel/bladder control. | Walking with KAFO and walker, sitting balance improved, trunk control improved, step taking better, uses condom catheter, sensation till left hip. |
| 81193 | Unable to walk or stand, loss of sensation below nipples, weak hand grip, partial bladder sensation but no control, no bowel control, abnormal sitting and standing balance. | Feels intermittent singling in B/L LE, stands and walks with KAFO calipers, sitting, standing posture and balance improved, B/L hand grip improved, feels pressure in lower limbs on standing, spasticity reduced. |
| 81194 | Patchy sensation below L1 region, partial bowel/bladder sensation but no control, poor sitting balance, unable to walk or stand. | Sitting balance improved, sensation in legs improved, motor strength improved, toe movements present (right > left). Left foot movement present, step taking improved, walks with KAFO caliper and walker. |
| 81206 | Not able to stand or walk, no movement in legs, no bowel/bladder control, no sensation below umbilicus. | Walks independently with knee caliper and walker, crawling are good, flicker movement in toes, patchy deep sensation present, good sitting balance. |
| 81215 | No sensation below lower neck, B/L upper limb weak grip, no movement in lower limbs, not able to sit without support, absent bowel/bladder sensation, bed sores present. | Stands with KAFO calipers and walker, sitting with support of ball, sensation same as before, bed sores healing. |
| 81216 | Loss of power and sensation in B/L and L/L, loss of bowel/bladder sensation, tingling, burning, deep pressure felt in B/L lower limb, deep sensation and bladder fullness perceived. | Mild flicker movement of toes, ankles (left > right), able to walk with walker, knee brace and AFO without any assistance, sensation improved. |
| 81223 | No motor sensation below the level of injury, bowel/bladder sensation and control absent unable to stand or walk. | Flicker in the B/L knee extensor, sensation improved good bowel/bladder sensation, stands and walks KAFO walker, core strength improved. |
| 81253 | No superficial sensation below injury level, no sensation in ankle and toes, hand grip weak, can stand on knee braces, cannot walk, full bowel/bladder sensation but no control. | Able to walk with KAFO and Walker and with little support, sitting and standing balance improved, right leg sensation improved, flicker movements in B/L lower limb muscles, toes and ankles, right side sweating present in upper body. |