Figure 1. (a) Magnetic resonance imaging shows a mass of 15 cm in diameter. Axial T1W image shows well-circumscribed solid and heterogeneous mesenteric mass. (b) It might seem to have an eccentric scar, although calcification could also be possible. It is difficult to discern by magnetic resonance imaging. (c) Axial T2W fat sat image shows a large mesenteric mass. Notice the slightly decrease of signal intensity and the lack of a peripheral capsule. (d) Gross aspect of the tumor was cyst, the outer surface was soft whitish, and focally presents yellowish adipose tissue of normal characteristics. (e) Cut surface showed cellular debris. (f) The cyst wall was thin and homogeneous.
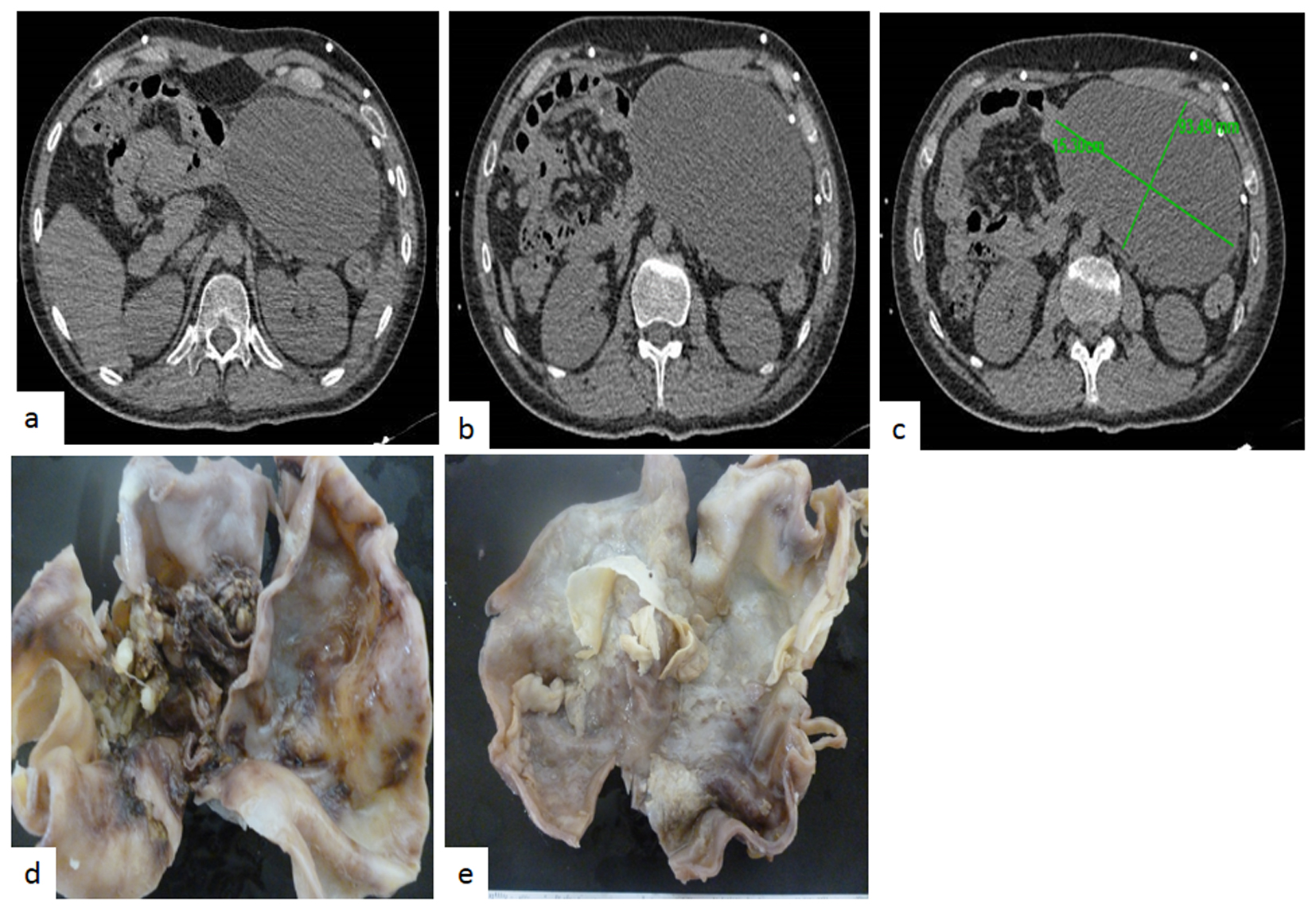
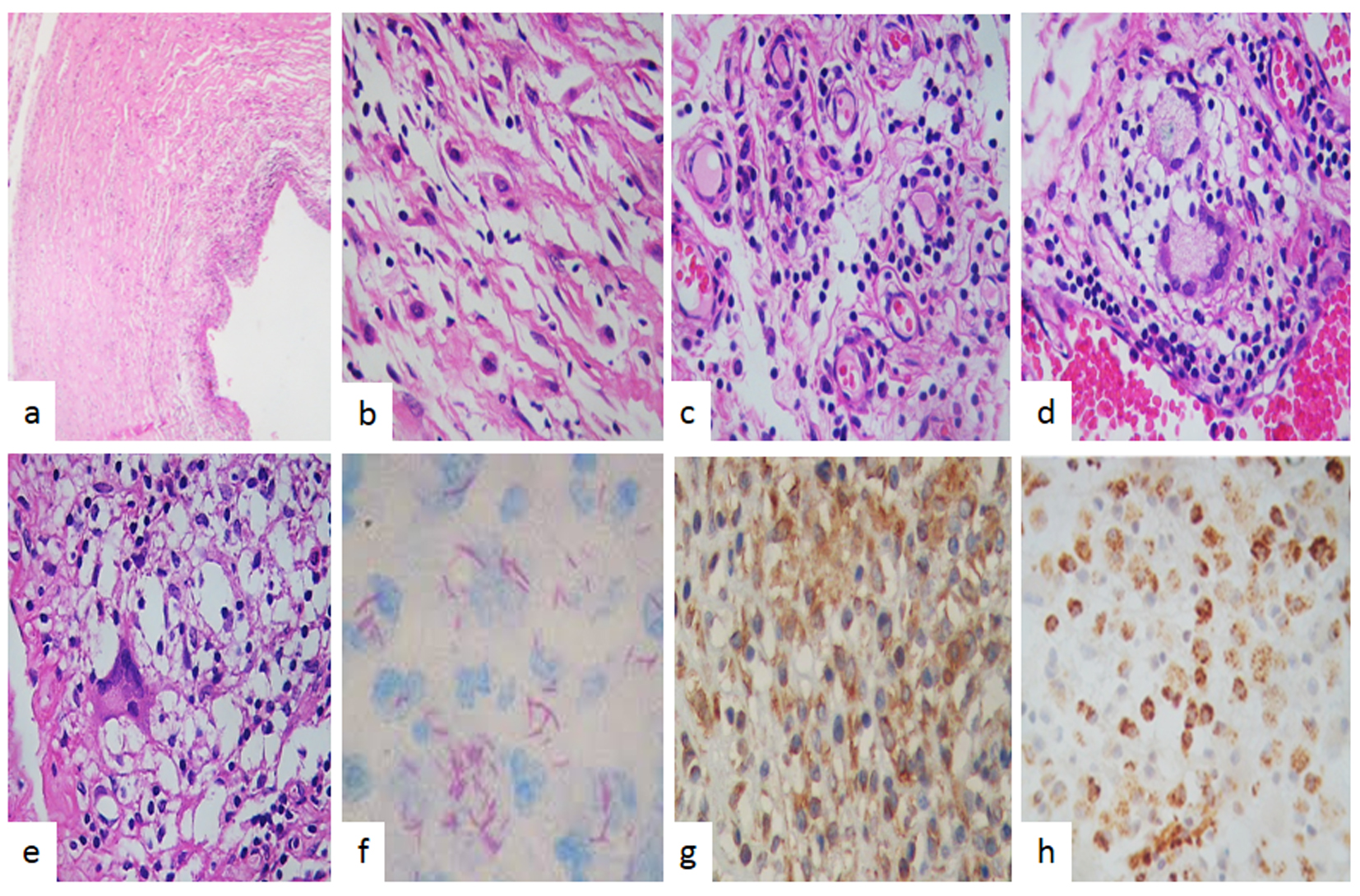
Figure 2. Pathologic findings. (a) Cyst tumor formed by spindle myofibroblastic cells in a fibromyxoid background with intermingled inflammatory cells (H&E, × 200). (b) High power examination revealed a fibroblastic and myofibroblastic proliferation with lymphocytes and plasma cells and macrophages without caseating necrosis. (c) Vessels proliferations, lymphocytes and macrophages were observed (H&E, × 400). (d) Giant cells and granuloma were also observed. (e) Giant cells and dirty macrophages that contained red bacillus, Zeel-Nielsen stain positive in (f). (g) Immunohistochemistry stain showed that spindle myofibroblastic cells were vimentin positive immunoreaction and in (h) observed that the most common cells were macrophages which were strong positive to CD68 (IHQ, × 400).