







| Journal of Neurology Research, ISSN 1923-2845 print, 1923-2853 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Neurol Res and Elmer Press Inc |
| Journal website http://www.neurores.org |
Case Report
Volume 2, Number 6, December 2012, pages 247-249
Arachnoid Cyst as a Rare Cause of Headache in a Teenager: Case Report
Hakan Aka, e, Ismail Gulsena, Gokhan Evcilib, Ugur Demirc, Sercan Savas Yalcind
aHakan AK, Bozok University, School of Medicine, Department of Neurosurgery, Turkey
bBitlis State Hospital, Neurology Clinic, Bitlis, Turkey
cBitlis State Hospital, Radiology Clinic, Bitlis, Turkey
dVan State Hospital, Neurosurgery Clinic, Van, Turkey
eCorresponding author: Hakan Ak, Bozok University, School of Medicine, Department of Neurosurgery, Turkey
Manuscript accepted for publication December 12, 2012
Short title: Arachnoid Cyst in Teenager
doi: https://doi.org/10.4021/jnr156w
| Abstract | ▴Top |
Headache is a common complaint in children and adolescents. Only minority percentage of headaches is associated with serious causative factors such as space occupying lesion. Arachnoid cysts compose less than of one percent of all intracranial lesions and they are mostly asymptomatic. Herein, we present a teenager with refractory headache diagnosed with arachnoid cyst. Cystoperitoneal shunt insertion was performed and patient’s complaint totally resolved.
Keywords: Arachnoid cyst; Headache; Computed tomography; Shunt
| Introduction | ▴Top |
Headache is one of the most common types of recurrent pain. This complaint constitutes a very high percentage of attendance to neurology as well as neurosurgery clinics. It is also common in children and it shows an increased prevalence during adolescence [1]. Most common causes of headache in children usually are not associated with serious causes such as space occupying lesion or life-threatening infection [2]. Arachnoid cysts compose only 1% of all intracranial space occupying lesions and most of them are asymptomatic. When they become symptomatic, they may create signs and symptoms according to their localization site [3]. Herein, we present a male teenager attended with only headache and diagnosed with arachnoid cyst. After cystoperitoneal shunt operation, patient’s complaint resolved in the early period.
| Case Report | ▴Top |
A 15-year-old male attended with only headache to our clinic. Pain was left sided (hemicranial) and was worsening in the morning. It was increased for recent times and it become resistant to easily accessible drugs such as paracetamol, naproxen, and diclofenac. There weren’t any accompanying symptom like nausea, vomiting, seizure, and loss of consciousness. There was no history of trauma or any infectious disease. Family history was unremarkable. Physical and neurological examinations were normal. Because of refractory headache, cranial computed tomography (CT) was taken and it revealed a left sided space occupying lesion isodens with cerebrospinal fluid and it was suppressing the frontal, temporal, and parietal lobes. Sulci were obscure at the left side. Left lateral ventricle was suppressed, and posterior horn of right lateral ventricle was enlarged due to probable compression of the foramen monro. Also, there was a midline shift (Fig. 1). This lesion was considered as an arachnoid cyst. It is type III arachnoid cyst according to Galasssi classification. Operation was planned due to suppression of neural structures, presence of midline shift, and absence of any reason to explain the patient’s headache. Cystoperitoneal shunt insertion that can be applied in most of the health centers was performed. Medium pressured automated antisiphon shunt material was inserted. Patient’s headache disappeared after operation even in the early period. Patient is still under clinic controls without any complaint for about one year.
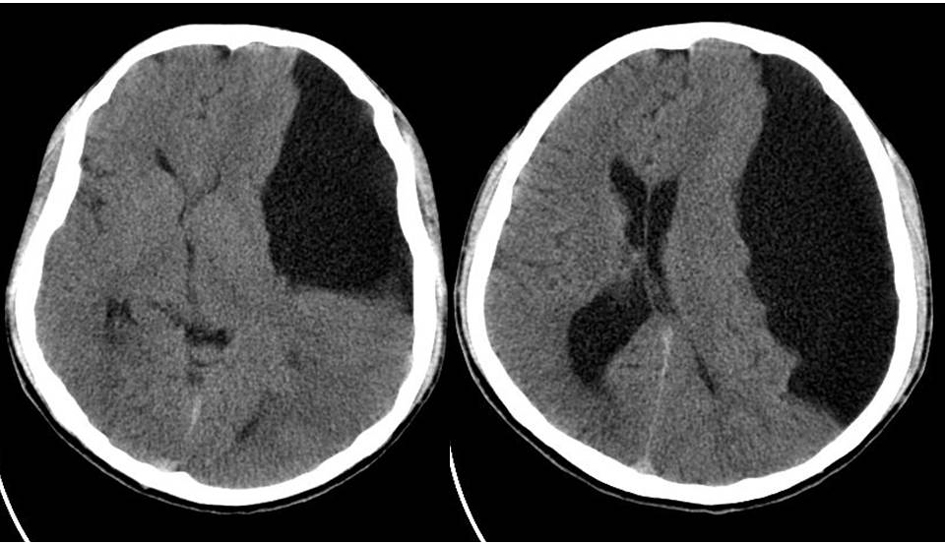 Click for large image | Figure 1. CT images showing the arachnoid cyst. There was midline shift and pressure on frontal, temporal, and parietal lobes. |
| Discussion | ▴Top |
As in adult patients, headache is also a common problem in children and frequency increases towards the adolescence. It was reported that prevalence of any type of headache range from 57-82% by age of 15 [1]. The most common causes of headache in children can be summarized as viral or upper respiratory infections including ear infections, common cold, allergies, sinus infections, and strep throat, stress-related or stress-worsened headaches including family or school problems, minor head injury, migraine or cluster headache, and tension. Only a small minority of children with headaches have a serious cause, such as a brain tumor or life-threatening infection [2].
The evaluation of patient with headache begins with thorough medical history followed by physical examination and complete neurological examination. Physical examination should include vital signs, particularly blood pressure, and neurological examination should include optic fundus [1]. The red flags in patients’ medical history were summarized as age < 3 years, morning or nocturnal headache, morning or nocturnal vomiting, headache increased by Valsava or straining, explosive onset, progressively worsening over time (chronic progressive pattern), declining school performance or personality changes, altered mental status, and epilepsy [4]. The red flags in physical examination are hypertension, head circumference more than 95%, neurocutaneous markers, meningeal signs, papilledema, abnormal eye movements, motor asymmetry, ataxia, gait disturbance, and abnormal deep tendon reflexes [4]. All of the physical examination red flags were negative in our patient. However, some of red flags were positive in our patient including, pain worsening morning, pain progressively worsening over time.
Although arachnoid cysts are considered as benign developmental malformation of the arachnoid membrane, it was also reported that head trauma during infancy may have a role in the pathogenesis [3, 5]. Arachnoid cysts are classified into groups according to their localizations. Most common localization site is the middle fossa which constitutes about 65-67%. The second most common localization is the posterior fossa compromising about 15-17%. Other localizations are suprasellar, frontal, cerebral convexity, interhemispheric fissure, and quadigeminal cistern. Most of these cysts are asymptomatic. However when these become symptomatic, they cause symptoms and signs generally according to their localization sites. Middle fossa arachnoid cysts are mostly manifested with headache, seizure, contralateral weakness, mental retardation, and behavioral disorder [3, 6-11]. The only complaint of our patient was headache worsening with over time.
Treatment of arachoid cysts is still under debate [9]. Surgical indications are increased intracranial pressure, progressive hydrocephalus, presence of pressure onto neural structures, refractory epilepsy which is confirmed to be due to cyst, and development of intacystic and subdural hemorrhage [9-12]. Our surgical indications include headache which was considered to be due to increased intracranial pressure, and presence of pressure onto neural structures. Current operative techniques for arachnoid cysts are microsurgical excision, insertion of cystoperitoneal shunt, endoscopic ventriculocystotomy, stereotactic cysto-venticular shunt insertion, and stereotactic intracavitary irradiation [13]. Each of these techniques has their own advantages and disadvantages. For example, microsurgical techniques have an advantage on not needing shunt during lifetime. However, this technique may not be always effective. Cyst may recur, and each of the operative morbidity such as meningitis, hemiparesis, oculomotor paralyse, subdural hematom, seizure, and even death may be seen. Cystoperitoneal shunt insertion is an easy and effective technique. It is the best option in infants and babies for complete obliteration of the larger cysts. However, shunt dependency, subdural hematoma, and shunt malfunction in the early and late period after insertion are disadvantages. Endoscopic procedures are also reliable. However, in these techniques, intra cerebral bleeding, intraventricular bleeding, and ventriculitis may be seen especially in the inexperienced hands [13]. Stereotactic intracavitary irradiation has been reported in limited cases. Regression of the cyst without any complication and symptomatic recovery has been reported with the use of this technique [14]. We performed CP shunt insertion which can be performed in most of the health centers easily. We gained good result even at the early period after operation. Use of automated antisiphon shunt prevented fast drainage and ultimately development of subdural hematoma.
In conclusion, in teenagers with refractory headache, the probability of the presence of arachnoid cyst should be kept in mind and arachnoid cyst can reach to surgical limits without any abnormal physical examination finding. We also can conclude that we should be careful about red flags in medical history and physical examination. In addition, cystoperitoneal shunt insertion is still an effective method in the treatment of these cysts due to relatively easy application and being applicable in most of the health centers.
Conflict of Interest
We have no conflict of interest.
| References | ▴Top |
- Lewis DW, Ashwal S, Dahl G, Dorbad D, Hirtz D, Prensky A, Jarjour I. Practice parameter: evaluation of children and adolescents with recurrent headaches: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2002;59(4):490-498.
doi pubmed - Bonthius DJ, Lee AG. Patient information: Headache in children. 04.11.2012. http://www.uptodate.com/contents/headache-in-children-beyond-the-basics.
- Choi JU, Kim DS. Pathogenesis of arachnoid cyst: congenital or traumatic? Pediatr Neurosurg. 1998;29(5):260-266.
doi - Lewis DW. Headaches in children and adolescents. Curr Probl Pediatr Adolesc Health Care. 2007;37(6):207-246.
doi pubmed - Helland CA, Wester K. A population based study of intracranial arachnoid cysts: clinical and neuroimaging outcomes following surgical cyst decompression in adults. J Neurol Neurosurg Psychiatry. 2007;78(10):1129-1135.
doi - Wester K. Peculiarities of intracranial arachnoid cysts: location, sidedness, and sex distribution in 126 consecutive patients. Neurosurgery. 1999;45(4):775-779.
doi pubmed - Passero S, Filosomi G, Cioni R, Venturi C, Volpini B. Arachnoid cysts of the middle cranial fossa: a clinical, radiological and follow-up study. Acta Neurol Scand. 1990;82(2):94-100.
doi pubmed - Arai H, Sato K, Wachi A, Okuda O, Takeda N. Arachnoid cysts of the middle cranial fossa: experience with 77 patients who were treated with cystoperitoneal shunting. Neurosurgery. 1996;39(6):1108-1112; discussion 1112-1103.
- Ibarra R, Kesava PP. Role of MR imaging in the diagnosis of complicated arachnoid cyst. Pediatr Radiol. 2000;30(5):329-331.
doi - Lutcherath V, Waaler PE, Jellum E, Wester K. Children with bilateral temporal arachnoid cysts may have glutaric aciduria type 1 (GAT1); operation without knowing that may be harmful. Acta Neurochir (Wien). 2000;142(9):1025-1030.
doi - Wang PJ, Lin HC, Liu HM, Tseng CL, Shen YZ. Intracranial arachnoid cysts in children: related signs and associated anomalies. Pediatr Neurol. 1998;19(2):100-104.
doi - Erman T, Gocer I, Tuna M, Ergin M, Zorludemir S, Cetinalp E. Intracranial arachnoid cysts: clinical features and management of 35 cases and review of the literature. Neurosurg Q 2004; 14: 84-88.
doi - Shim KW, Lee YH, Park EK, Park YS, Choi JU, Kim DS. Treatment option for arachnoid cysts. Childs Nerv Syst. 2009;25(11):1459-1466.
doi pubmed - Thompson TP, Lunsford LD, Kondziolka D. Successful management of sellar and suprasellar arachnoid cysts with stereotactic intracavitary irradiation: an expanded report of four cases. Neurosurgery. 2000;46(6):1518-1522; discussion 1522-1513.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Neurology Research is published by Elmer Press Inc.